
Skin Cancers
Skin cancers are increasingly common. There are 3 main types, basal cell carcinoma (BCC or rodent ulcer), squamous cell carcinoma (SCC) and melanoma. Most skin cancers are related to sun exposure, although this does not mean that only sun-bathers get them. The different types of skin cancers have different features, most are relatively straightforward to cure, but a few are more concerning.
Please click on the links below for further information.
BCC is a very common type of skin cancer. In most cases it is much less serious than other cancers, and can usually be cured with relatively simple treatment. BCC mostly affects fair skinned people, on sun-exposed areas, particularly the face and scalp. BCC is caused by sun damage to the skin. You do not need to be a sun worshiper to develop BCC, even ordinary day to day sun exposure over many years can lead to this type of skin cancer.
BCCs start as either a small ulcer or scab that may bleed or weep from time to time, or as a smooth, raised pink or pearly looking growth on the skin. BCCs usually grow slowly. If this type of growth is ignored, it may develop into a large ulcer; this is sometimes called a rodent ulcer.
The diagnosis is usually made on the examination in clinic. In some cases where the diagnosis is not clear, a biopsy may be required. A biopsy involves taking a small sample from the lesion after numbing the area with local anaesthetic injections; this is usually done in the outpatient clinic where there is a minor operating theatre.
Treatment
Most BCCs are treated by surgical excision. Alternative treatments are radiotherapy, and for smaller, superficial lesions, cryotherapy, curettage or prescription creams.
Surgical excision
Surgical excision means cutting the growth out. This is done usually with local anaesthetic injections to numb the area first. Removal of larger BCCs or when the surgery is more technically involved, may need to be done under general anaesthetic. The BCC is excised as an ellipse shaped strip, and the wound edges stitched, when this is possible. When a larger growth has been excised, if there is not much loose skin, or if the BCC is near to the eye or mouth, it may not be possible to stitch the resulting wound, and plastic surgery reconstruction is required.
Any suspected skin cancer that is excised will be sent to the pathologist to establish the diagnosis. Pathology results take about a week. One of the advantages of surgical excision of a skin cancer is that the diagnosis and completeness of excision is known; with other techniques (radiotherapy, cryotherapy, curettage) there is less certainty that the treatment has been adequate.
Reconstruction

There are 2 main techniques of plastic surgery reconstruction, skin graft or local skin flap. A skin graft is a piece of skin taken from another part of the body, placed on the wound which it grows on to. The skin graft may be either a split skin graft, a very thin shaving of skin usually taken from the leg or arm, or a full thickness skin graft which it a thicker piece of skin taken from behind the ear, above the collar bone or groin. A split skin graft leaves a wound similar to a graze, and this takes 2 or 3 weeks to slowly heal. The choice of which type of skin graft is used depends on the size and location of the wound; full thickness skin grafts are more often used on the face, split skin grafts on the scalp.
A skin flap involves moving a piece of skin from one side of the wound in order to allow the wound to be stitched. This technique is particularly useful near the eye or mouth, or on the nose. Additional cuts are required when doing a skin flap reconstruction.
Skin cancers frequently involve the face. Curative treatment is essential, but an excellent cosmetic result is also very important. As a Plastic Surgeon, I will ensure the best possible cosmetic outcome. I pride myself on meticulous surgical technique, founded on extensive experience.
Radiotherapy
Radiation treatment is an alternative to surgical excision. Radiotherapy is a course of treatments spaced over 1-2 weeks usually. An X ray beam is used to destroy the cancer cells. The treatment will make the area sore during and after the treatment. When the area has healed completely (this takes several weeks), there is some scarring and colour change of the skin.
Radiotherapy is chosen for large or indistinct lesions, when surgical treatment is difficult, or for patients who cannot have surgery for medical reasons.
Cryotherapy
Cryotherapy uses a freezing spray to destroy the cancer cells. It is only suitable for small, superficial BCCs. The treatment is done in the clinic and only takes a few minutes. The area treated turns into a scab which takes a couple of weeks to separate. You will be seen again in the clinic to check the BCC has been adequately treated.
Prescription creams
There are 2 creams that may be used to treat superficial BCCs, Imiquimod and Effudix. The course of treatment is several weeks. The area will become red and sore during the treatment. You will be seen again in the clinic to check the BCC has been adequately treated.

SCC is much less common than BCC and tends to affect elderly people. SCCs appear as ulcerated lesions, moist or crusty growths from the skin. SCCs are more common in sun exposed areas, such as the face, scalp or hands, but may occur in any part of the body. SCCs often start as a red scabby patch of skin that is an area of sun damage, which becomes ulcerated or gets bigger, often quite rapidly.
SCCs have the potential to spread to other parts of the body (metastasize), however this is relatively uncommon. The lymph glands are checked, as SCC can spread to these.
Treatment
SCC is usually treated by surgical excision. The growth is removed with a 'safety margin' (about 5mm) of normal looking surrounding skin. The resulting wound is either stitched, or with larger lesions and lesions at certain sites, reconstruction using plastic surgery techniques of local skin flap or skin graft (see under BCC).
Radiotherapy is an alternative treatment; this is considered for larger growths, and those that are not suitable for surgery either because of their site, or if the patient cannot have surgery for medical reasons.
Solar keratosis (also called actinic keratosis) is a scabby or raw area caused by sun damage to the skin. These areas may ulcerate or bleed. Sun damage causes a spectrum of skin lesions, solar keratosis is the earliest change, this may progress to Bowen's disease, a precancerous condition, and the most severe change is SCC. An experienced specialist is often able to make the diagnosis of solar keratosis by careful examination, however if there is any question of the diagnosis a biopsy is required.
Treatment
Solar keratosis may be treated with a cream called Effudix, with cryotherapy, or by surgical excision.
Keratoacanthoma (KA) is similar to SCC in appearance. It is a cone shaped crusty growth with a black scab in the centre (it looks a bit like a little volcano). KA develops quite rapidly. The peculiar feature of KA is that the growth may disappear within a few months; this is known as involution. Because of this, a lesion that is a typical KA may be observed, to see if it starts to involute. If this does not occur within a few months, surgical treatment is necessary. A biopsy may be advised to help establish the diagnosis.
Treatment
KA may be closely observed and allowed to involute. Surgical treatment is either curettage (scraping away the growth with a special instrument), or complete excision; both of these treatments are done with local anaesthetic.
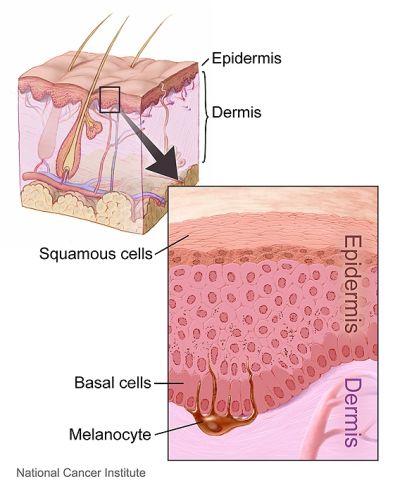
Melanoma is a skin cancer that arises from the pigment cells in the skin (melanocytes), and because of this, melanoma is darkly pigmented (brown, blue or black). Melanoma has the potential to spread to other parts of the body (metastasize), and needs prompt and expert treatment.
Melanoma occurs usually in fair skinned people, and at any age from late teens onwards. We know that melanoma is related to sun exposure (although you do not need to be a sun-worshiper to develop melanoma). Melanoma may occur at any part of the body, including areas that are not exposed to the sun, even the soles of the feet.
Any mole that appears where there was previously not one, or a mole that changes significantly over a short period should be checked by a specialist (a plastic surgeon or dermatologist). it is a good idea to have a mole checked if it changes in any of the following ways:
- gets larger over a short period, particularly if it is more than 5mm across
- becomes raised when it was previously flat
- the shape changes or becomes irregular (healthy moles generally have a roundish shape and smooth outline)
- bleeding or ulceration
- gets darker in colour or the colour is irregular (patches of dark brown / black / red)
In most cases it is possible to reassure you about a mole after carefully examining it. In some cases, biopsy may be required. Biopsy can be done in the minor treatment room at my Chelsea Outpatient Centre and Syon BMI clinics.
A biopsy involves taking a sample of the lesion (sometimes the whole lesion is removed), and this is sent to the pathologist who analyses it. Results usually take 3-4 days.
Treatment
The treatment of melanoma depends on the site, size and stage. Stage is how advanced the melanoma is, and this is determined by the pathology (particularly how deeply the melanoma cells extend, called thickness), and whether there is evidence that the melanoma has spread.
The melanoma is treated by surgical excision, with a 'safety margin' of normal looking skin around it, usually 1cm. Because a larger piece of skin and tissue needs to be removed, it may not be possible to stitch the wound edges, and reconstruction using plastic surgery techniques (most often a skin graft) will be required in this case.
Patients with advanced melanoma, particularly when the disease has spread, are referred to a specialist centre where addition treatment is available.
Monitoring
Patients who have had a melanoma are followed up closely for a period of 5 years. This is because melanoma can recur, either near to the original site (local recurrence) or some where else in the body (regional recurrence or metastatic disease). You will be asked if you have lost weight or have any unexplained symptoms, for example yellowness of the eyes (jaundice), and whether there are any new moles that have appeared. I check the site where the melanoma was removed, and the nearest group of lymph glands. If you have any concerns, you should arrange to see your specialist immediately, not wait for the next scheduled appointment.